Studies have reported pre-eclampsia, fetal growth restriction, pre-term delivery, fetal demise and spontaneous miscarriage to be associated with abnormal deviations in either one or
several components of biological and immune markers. In low and middle-income countries,
approximately 13.7 million babies are born preterm and 32.4 million are born small for
gestational age out of which 2.8 million are born both preterm and SGA. These infants have been shown to be at an increased risk of high morbidity, neonatal and infant mortality as well as long-term disability such as increased risk of neurodevelopmental disorders. Further
information on a range of risk factors implicated in these pathophysiologies is needed and warrants further research. Centre for Public Health Kinetics is part of a three country Alliance for Maternal and Newborn Health Improvement study whose main aim is to elucidate the
distribution of various fetal outcomes preterm -SGA, preterm-AGA, term-SGA and term AGA. We also aim to study the association of maternal and epidemiological risk factors for these outcomes across four countries in Asia and Africa.

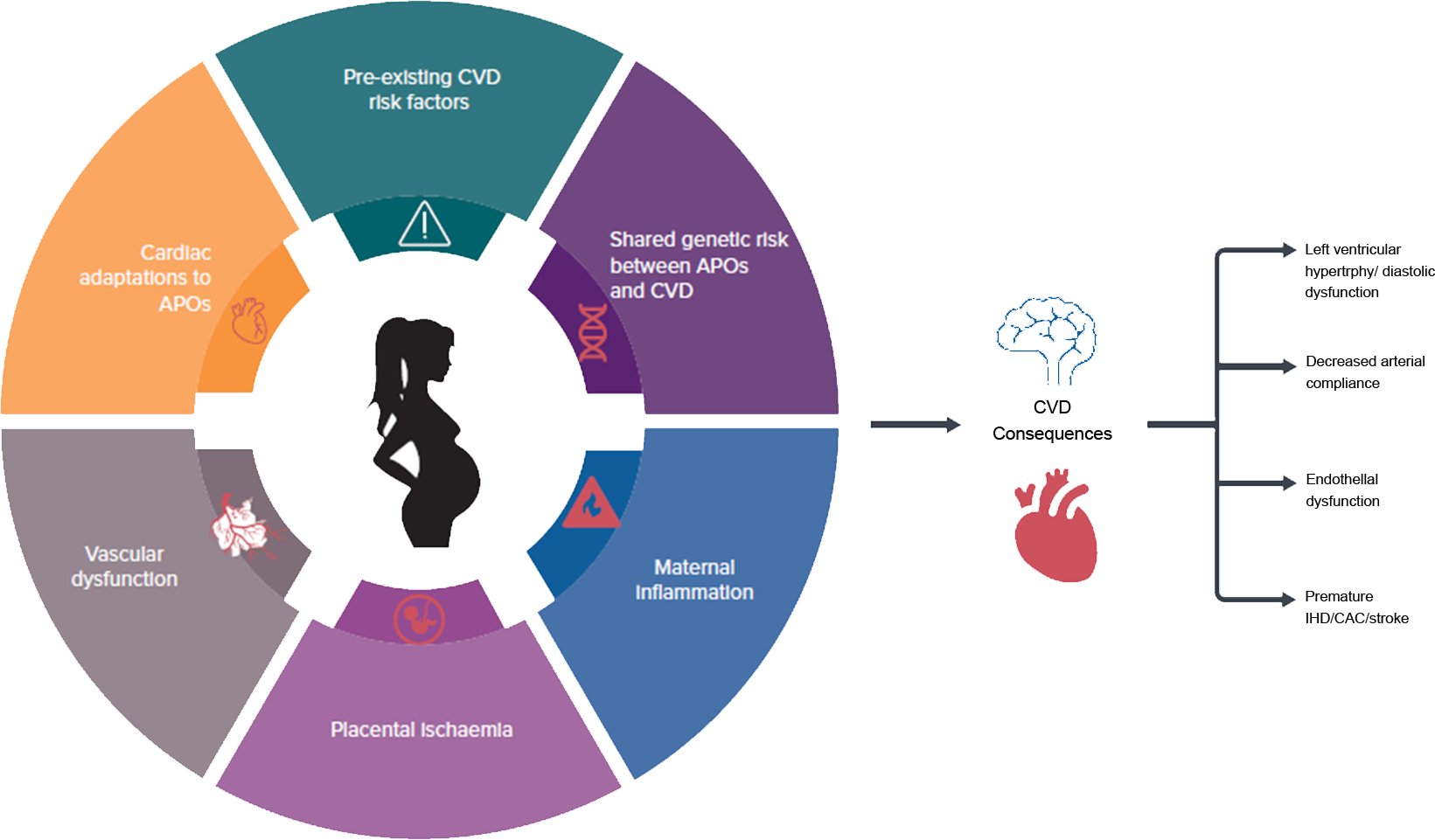 The burden of adverse pregnancy outcomes is substantial in both developed and developing countries (Lee et al, 2013; Beck et al, 2010; Blencowe et al, 2012). More than 60% of preterm births take place in south Asia and sub-Saharan Africa (Blencowe et al, 2012). APO is a complex, multi-factorial, physiological outcome in women, and despite decades of research, a clear causal mechanism for these adverse outcomes has not been established.
The burden of adverse pregnancy outcomes is substantial in both developed and developing countries (Lee et al, 2013; Beck et al, 2010; Blencowe et al, 2012). More than 60% of preterm births take place in south Asia and sub-Saharan Africa (Blencowe et al, 2012). APO is a complex, multi-factorial, physiological outcome in women, and despite decades of research, a clear causal mechanism for these adverse outcomes has not been established.  While India has made significant progress for reducing under five mortality in the last decade, efforts are still being undertaken by the government to achieve the 3rd Sustainable Development Goal of
under-five mortality of 25 per 1000 live births by 2030. As per the National Health Policy, the effort is also to reduce
neonatal mortality to 16 by 2025 and to address malnutrition by reduction of 40% in prevalence of stunting of under 5
children by 2025.
While India has made significant progress for reducing under five mortality in the last decade, efforts are still being undertaken by the government to achieve the 3rd Sustainable Development Goal of
under-five mortality of 25 per 1000 live births by 2030. As per the National Health Policy, the effort is also to reduce
neonatal mortality to 16 by 2025 and to address malnutrition by reduction of 40% in prevalence of stunting of under 5
children by 2025.